|
Formation of a Spinal Nerve 1. outer white matter 2. inner grey matter 3. dorsal horn is sensory unipolar neurons concerned with general sensation which have receptors peripherally. 4. ventral horn is motor multipolar neurons which synapse with effector organ 5. dorsal and ventral roots unite to form a spinal nerve
|

|
1. spinal n. has two major branches which are the dorsal and ventral primary rami (mixed nerves)
2. dorsal primary rami innervate: -deep muscles of the back -dermatomes of posterior surface of neck and trunk
3. ventral primary rami innervate everything else: -all the skin and muscles of the UE and LE -s/f muscles of the back -remaining muscles and lateral/anterior dermatomes of the trunk. |
| 31 pairs |
|
Epicritic: precise and pinpoint 1. fine touch 2. proprioception (muscle/tendon stretch and tension) 3. vibration
Protopathic: diffuse but quick as ascends to CNS. 1. Pain (fast acute & slow chronic) 2. Temperature
|
|
Motor AND sensory
Sensory receptors are associated with epicritic proprioception: -Muscle spindles are stretch receptors in muscle. -Golgi tendon organs are tension receptors in tendons. |
|
1. loss of all sensation. anesthesia
2. without pain. analgesia
3. ability to recognize an object through sense of touch without visual cues (this is of which modality?). stereognosis (epicritic)
4. related to movement, perception of angle of joint, and relative weight of objects. Kinesthesia |
|
1 - analgesia is related to what modality? protopathic
2-astereognosis and akinesthesia are related to what modality? epicritic |
|
Sensory neurons 1. of which root, type of neuron. - dorsal root, unipolar
2. innervate what 2 structures - skin (dermis/epidermis for pain, touch, temp, and pressure)
-skeletal muscle (stretch and tension)
|
|
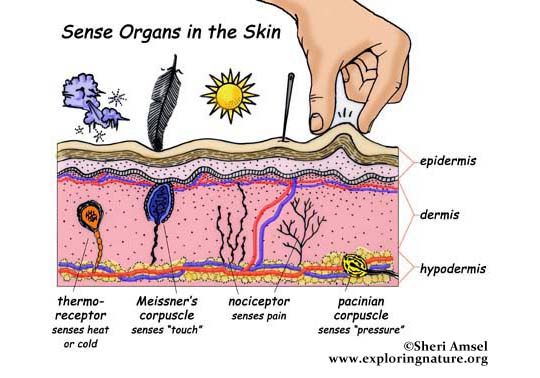
Sensory Receptors in Skin 1. innervate what 2 layers - epidermis and dermis 2. naked nerve endings - nociceptors (pain receptors) 3. Pacinian Corpuscle - associated with pressure sense
Sensory receptors in Skeletal Muscle 1. receptor of stretch/length - muscle spindles IN MUSCLE 2. receptors of tension - golgi tendon organ (GTO) IN TENDONS |
|
-1º Neuron 1. unipolar 2. cell body location - dorsal root ganglion 3. peripheral process (part that goes to the skin) associated with a a receptor that responds specific stimulus 4. central process enters the spinal cord via the dorsal root 5. synapses where? - CNS (spinal cord or brain stem depending on modality) 6. Entire 1º neuron is unilat (located on 1 side of body)
-2º Neuron 1. cell body location - CNS (spinal cord or brain stem depending on modality) 2. **axon immediately decussates to contralat side ¨this is definitely on test, bitches¨ - Dr. H 3. ascends in CNS via long ascending tract (tract in brain and spinal cord form white matter = bundles of myelinated axons). 4. Synapses where? - thalamus
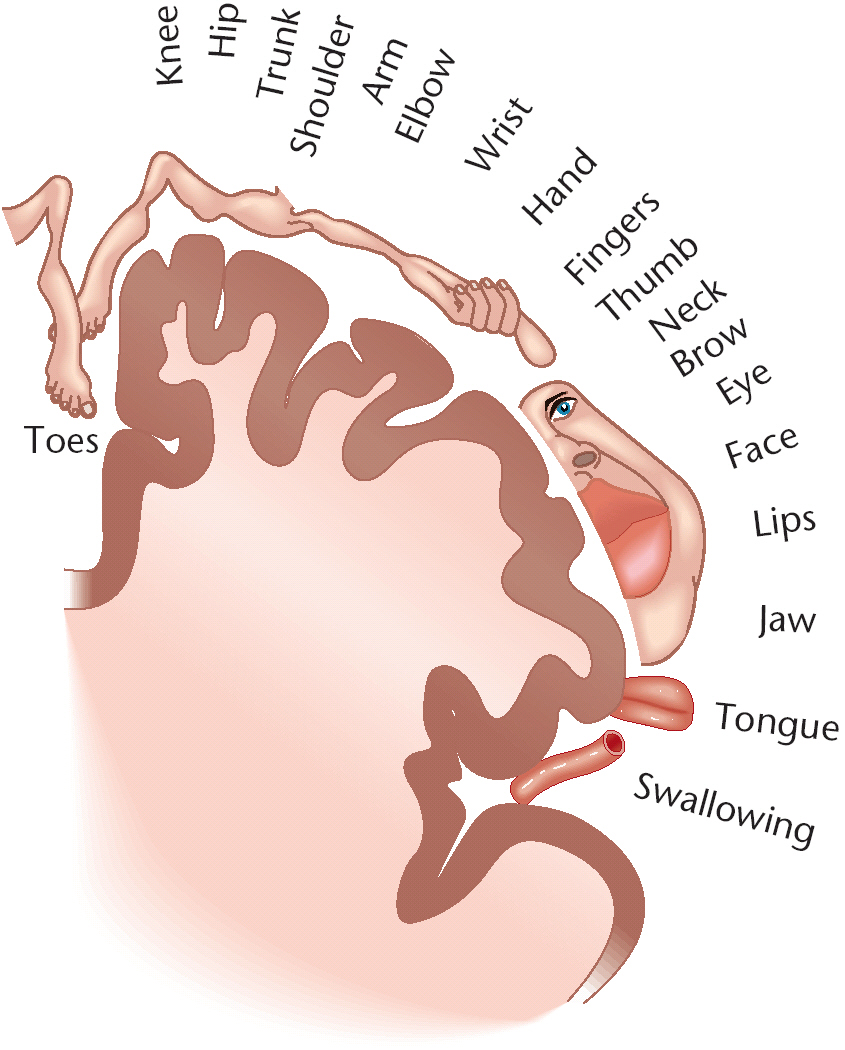
-3º Neuron 1. cell body location -thalamus 2. axon ascends via posterior limb of the internal capsule 3. synapses in the postcentral gyrus & paracentral lobule of the parietal lobe in the somatosensory cortex for general sensation.
|
| Tract |
|
1. Largest structure in diencephalon of the brain. 2. Serves as a relay center to/from cerebral cortex. 3. Grey matter existing bilaterally. 4. Location of 3º neuron and the synapse of 2º neuron of general sensory pathways.
|


|
area 3,1,2 which is the somatosensory cortex (comprised of laterally, the postcentral gyrus and medially, the posterior paracentral lobule of parietal lobe)
|

| paracentral lobule |
|
EPICRITIC PATHWAY:
Faciculus Gracilis (recieves epicritic info from T7 and below) & Fasiculus Cuneatus ( from T6 and above) contribute to dorsal white matter of spinal cord, aka dorsal column, which are the axons of the primary neuron which ascend in spinal cord and synapse in medulla. |
|
EPICRITIC PATHWAY:
Bundles of 2º neuronal axons of the epicritic pathway which begin in the medulla and immediately decussate to contralateral side to ascend through the pons, midbrain, and synapse in the thalamus |
|
Stimuli from 1º neuron enter the dorsal column white matter of the spinal cord, comprised of the fasciculus gracilis (which recieves stimuli from T7 and below) and the fasciculus cuneatus (which recieves stimuli from T6 and above).
2º neurons begin in the medulla and immediately decussate to contralateral side via bundles of axons called the medial lemniscus. The information ascends through the pons and midbrain and synapses in the thalamus.
3º neurons then coarse through the posterior limb of the internal capsule to AREA 3,1,2 aka somatosensory cortex.
|


|
1. Contralateral 2. Ipsilateral neurological deficit from below the level of injury. |
| The site of the lesion. |
| C1 is only a motor nerve, there is no dermatome. |
|
1. Spinal Protopathic Pathway modalities - pain, temperature, crude touch 2. fast/acute pain tract - lateral spinothalamic tract (LST) 3. slow/chronic pain tract - anterior spinothalamic tract (AST) |
|
1.DECUSSATION -Protopathic: segmental decussation at every level in the spinal cord via anterior white commisure, specifically the level in which it is recieved. -Epicritic: decussates in medulla via medial lemniscus.
2. 1º neuron synapse -Protopathic: synapses in dorsal horn of gray matter -Epicritic: synapses in medulla
|
|
Pain, temp, and crude touch stimuli from 1º neuron synapse in dorsal (posterior) horn.
2º neuron decussates and the same spinal level from which is was recieved via the anterior white commisure and ascends via the lateral spinothalamic tract (fast/acute pain and temp) or anterior spinothalamic tract (slow, chronic pain and crude touch) and synapses in the thalamus.
3º neuron ascends through pons, midbrain, and coarses through posterior limb of internal capsule to AREA 3,1,2 aka somatosensory cortex.
|

| Thalamus (vs. cortex for epicritic pathways) |
|
1. a lesion in the L posterior limb of internal capsule results in... R (contralateral) loss of general sensation (both epicritic and protopathic modalities).
2. a lesion in the L pons results in... R (contralateral) loss of general sensation (both epicritic and protopathic modalities.
3. A L hemi-lesion in 1 level of the spinal cord results in... L (ipsilateral) loss of epicritic modalities & R (contralat) loss of protopathic modalities BELOW THE LEVEL OF INJURY |
|
1. LMN: multipolar neurons directly synapsing on voluntary skeletal muscle. Only motor neurons that innervate skeletal muscle. -injury=flaccid paralysis
2. UMN: neurons associated with motor cortex and brainstem, and synapse on LMN. -injury=spastic paralysis 3. Basal Ganglia: grey matter bilaterally, subcortical structures (no conscious awareness), neurons which influence activity of UMN. Contribute to posture, gross movements. -injury=dyskinesia (eg. parkinsons)
4. Cerebellum: reflex center for controlling the coordination of voluntary movement. Subcortical. Influence of UMN. -injury=ataxia (lack of coordination)
|
|
1. spastic paralysis - upper motor neuron 2. flaccid paralysis - lower motor neuron 3. dyskinesia - basal ganglia 4. ataxia - cerebellum |
|
Alpha motor neurons: 1. type of motor neuron - LMN
2. innervation - extrafusal skeletal muscle fibers, aka muscle cells, which control muscle contraction across a joint.
3. physical characteristics - large, heavily myelinatied multipolar neurons
4. conduction velocity - fast
5. location - all spinal nerves and all cranial nerves but I, II, VIII (olfactory, optic, vestibulocochlear are only sensory). |
|
Gamma motor neurons: 1. type of motor neuron - LMN
2. innervation - intrafusal skeletal muscle fibers, which are special fibers within muscle spindle that maintain the spindle as an effective stretch receptor.
3. physical characteristics - myelinatied multipolar neuron, not as large as gamma.
4. conduction velocity - slower than alpha (b/c less myelin).
5. location (same as alpha) - all spinal nerves and all cranial nerves but I, II, VIII (olfactory, optic, vestibulocochlear are only sensory). |
|
¨Oh Oh Oh, To Touch And Feel A Girl's Vagina, Ah Heaven¨
I - Olfactory - Purely Sensory Sense of smell
II - Optic - Purely Sensory vision
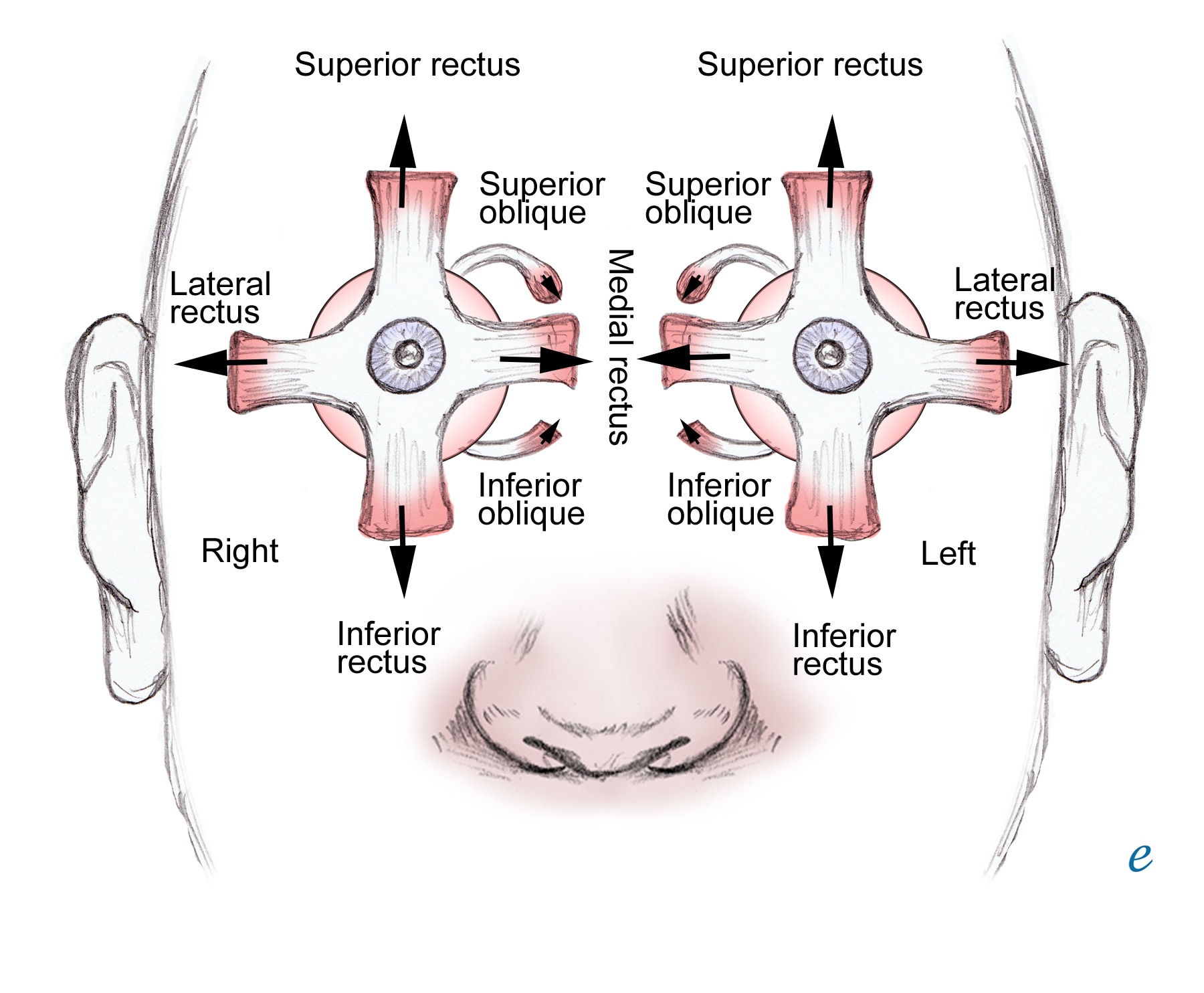
III - Oculomotor Levator palpebrae (eyelid open) Focusing (Iris/Lens) EOMs: SR, MR, IR, IO. *CNIII Palsy=Down n Out
IV - Trochlear EOM: SO
V - Trigeminal Muscles of Masticating Sensory of scalp, face, teeth
VI - Abducens EOM: LR
VII - Facial Expression Salivation Taste from ant 2/3 of tongue
VIII -Auditory (Vestibulocochlear) - Purely Sensory Posture, Balance, Equilibrium Hearing
IX - Glossopharyngeal Swallowing Taste from posterior 1/3 of tongue General Sensation from pharynx & throat
X - Vagus Visceral Muscle Movement Visceral Sensation
XI - Accessory Swallowing Trapezius & SCM
XII - Hypoglossal Movement of Tongue
|

| Reflex |
|
1. What receptor? Muscle Spindle Stretch receptor (proprioceptor) within the muscle (which stretches when you tap the patellar tendon)
2. What and where is the sensory neuron? 1º neuron of epicritic pathway which enters the dorsal horn
3. Where is the synapse between sensory and motor neurons? integrating center 4. Where is the cell body location of the motor neuron? motor cell body in ventral horn of spinal gray matter, its axon goes out ventral root, enters spinal nerve, and goes back to CONTRACT muscle that stimulus came from.
5. What happens to the antagonistic muscle? (in this case the hamstring). It relaxes. |
| Testing sensory neuron function, motor neuron function, and muscle function. |
|
1. occur when? with excessive tension on muscle tendon - it is a protective reflex
2. what is the receptor? golgi tendon organ in the tendon (proprioceptor)
3. receptor innervation sensory 1º neuron of epicritic system which enters spinal cord via dorsal horn
4. what connects sensory and motor neuron? Interneuron of the integrating center
5. what is the motor response? RELAXES effector muscle (and contracts antagonistic muscle) |
|
1. involves what sensory pathway? protopathic pathway (pain, temp) - a protective reflex
2. What is the receptor and its innervation? Nociceptor innervated by 1º neuron of protopathic pathway.
3. What is the motor response? contracts many effector muscles to withdrawal from the pain.
4. What happens to stabilize the body during the withdrawal reflex? crossed extensor reflex acts to stabilize the contralateral side of the body. |
|
LMN disease is characterized as flaccid paralysis
1. status of voluntary muscle (2) -paralysis -paresis 2. Muscle tone (4) -absent -hypotonicity (decreased) -fasciculations (occur 1st, mini twitches) -fibrillations (occur later, inobservable)
3. Status of superficial and deep reflexes (2) -areflexia -hyporeflexia
4. effects of lesion -limited to skeletal muscles directly innervated by involved LMN
5. lesion location (2) - CNS (cell body or axons) - peripheral nervous system (rootlets and peripheral nerves, damage is less reversible)
6. types of injury (3) - trauma - CVA - poliomyelitis |
| Poliomyelitis is a disease of LMNs |
|
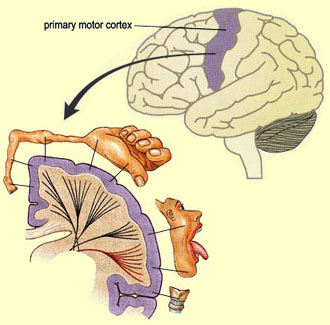
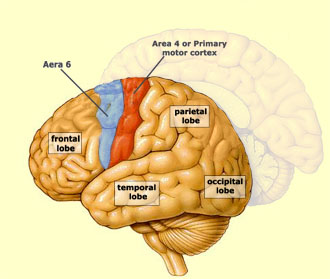
Primary Motor Cortex 1. aka AREA 4
2. location precentral gyrus (laterally) and anterior paracentral lobule (medially) of the FRONTAL lobe.
3. what is directly posterior to this region? Somatosensory Cortex (AREA 3,1,2) located in the postcentral gyrus and posterior paracentral lobule of the PARIETAL LOBE
|
|
1. innervation of upper extremity - Cervical Enlargement (Brachial Plexus)
2. innervation of lower extremity - lumbar and sacral enlargement
3. motor tract of UE & LE - corticospinal tract
4. motor tract of head region. concerned with synapsing what? corticobulbar tract synapses LMNs from brainstem to cranial nerves.
|

|
Corticospinal Tract 1. UMN synapse on LMN in the spinal cord 2. cortex is connected to contralateral side 3. from cortex to cord, system is located close to the peripheral surface, easily injured in trauma
|
|
1. Epicritic Pathway - sensory: fine touch, proprioception, vibration
2. Protopathic Pathway - sensory: pain, temp
3. UMN of corticospinal tract - motor |
| Injury to the internal capsule will NEVER cause LMN disease. *Only the UMN coarses through posterior limb of internal capsue = UMN disease. |
|
1. aka - pyramidal tract
2. From the motor cortex, the upper motor neuron coarses through the posterior limb of the internal capsule en route pyramids of the medulla
3. where does the decussation occur? pyramidal decussation in the medulla involves about 85% of the fibers, which descend via lateral white matter (lateral corticospinal tract) of the spinal cord
4. where do the fibers that don't decusatte descend? anterior corticospinal tract of spinal cord (which decussate later) not on exam
5. where does the synapse with LMN occur? spinal gray matter |
|
UMN Disease is characterized as spastic paralysis
1. Status of voluntary muscle (2) -paralysis -paresis 2. Muscle tone -hypertonicity (rigidity, increased tone)
3. Superficial Reflex status -Babinski sign - dorsiflexion and fanning of the toes (this is normal for prewalking child b/c corticospinal tract is not complete) 4. DTR Status -hyperrefflexia (¨clonus¨)
5. Effects of lesion Removes voluntary skeletal control inferiorly from the point of lesion.
6. lesion location CNS
7. types of injury (4) -Trauma -CVA -Tumors -Demylinating Disease (MS) |
|
A babinski sign (dorsiflexion and fanning of the toes) is indicative of what disease? UMN Disease In what population of patients is this a normal response? Children in pre-walking stage b/c the corticospinal tract has not fully developed yet. |
|
Is it UMN or LMN disease?
1. peripheral nerve/rootlet injury - LMN 2. injury to post limb of internal cpsule - UMN 3. CVA - UMN or LMN 4. Multiple Sclerosis - UMN 5. Poliomyelitis - LMN 6. Tumors - UMN 7. Trauma - UMN or LMN 8. A lesion in the CNS - UMN or LMN
|

|
R-sided Lesion of the posterior limb of the internal capsule results in CONTRALATERAL motor and sensory neuro deficits.
Left-sided... a) spastic hemiplegia - Corticospinal tract UMN b) loss of all general sensation - Epicritic (medial lemniscus) & Protopathic pathways
|

|
L-sided lesion of the pons (part of brainstem) results in CONTRALATERAL motor and sensory neuro deficits. Right-sided... a) loss of fine touch, DTRs, & vibration - Epicritic (medial lemniscus) b) loss of pain and temp sensation - Protopathic pathway c) spastic hemiplegia - Corticospinal tract UMN
|

|
L-sided hemi-lesion of the L1 spinal segment results in IPSILATERAL epicriticand UMN deficits & CONTRALATERAL protopathic deficits BELOW THE LEVEL OF INJURY.
Waist and below... a) L sided loss of fine touch, DTRs, & vibration-Dorsal column system (epicritic) b) R sided loss of pain and temp sensation-spinothalamic tract (protopathic) c) L sided spastic paralysis-corticospinal tract (UMN)
Example of a hemi-lesion (although this is at a higher level.
sensory loss related to spinal segments L1 and below.
Motor loss of L1 and below results in spastic paralysis. |



|
1. a lesion in the posterior limb of internal capsule -Corticospinal Tract (UMN): contralateral spastic hemiplegia -Contralateral loss of ALL general sensation (epicritic & protopathic)
2. a lesion in the pons (brain stem) -Medial Lemniscus: contralat loss of epicritic modalities (fine touch, proprioception, vibration) -anterior & lateral spinothalamic tracts: contralat loss of protopathic modalities (pain & temp) -Corticospinal Tract (UMN): contralat spastic hemiplegia
3. a hemi-lesion of a spinal segment Losses below level of injury: -dorsal column: ipsilat loss of epicritic modalities -spinothalamic: contral loss of protopathic modalities -corticospinal (UMN): ipsilateral spastic paralysis
|


|
When all the LMNs to a muscle group are injured, you will clinically be able to see THAT SPECIFIC muscle group having flaccif paralysis.
Eg: Assume we have a Lesion that affects 3-4 spinal segments of anterior horn, which damages MANY of motor neurons: Ipsilat flaccid paralysis for affected muscles, Everything else has spastic paralysis
*If you just have a small injury (a few LMN injured), clinically you cannot detect flaccid or spastic paralysis.
|
|
1. Corticospinal Tract: UMN and LMN 2. Neuro deficits: -LMN = ipsilat flaccid paralysis of muscle groups corresponding to affected spina segments. -UMN = ipsilateral spastic paralysis inferior to the affected spinal segments
|
|
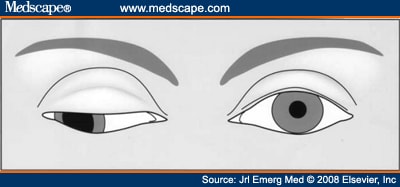
CST and CNIII injury:
1. Contralat Spastic Hemiplegia (UMN - SCT)
2. Ipsilateral Flaccid Paralysis (LMN - CNIII) of SR, MR, IR, IO extraocular muscles, levator palpebrae superioris (upper eyelid), and CNIII parasympathetic loss (pupil constriction & accomidation).
This results in CNIII palsy= down and out eyeball with dilated pupil.
|
|
CST and CNVI (Abducens) injury:
1. Contralat spastic hemiplegia (UMN- CST)
2. ipsilateral flaccid paralysis of lateral rectus muscle (LMN- CNVI Abducens)
|

|
CST and CNXII (hypoglossal) injury:
1. Contralateral Spastic Paralysis (UMN - CST)
Note the wasted left side of the tongue and deviation to the left suggesting a left lower motor neurone lesion. |

|
Right-sided lesion causing INFERIOR ALTERNATING HEMIPLEGIA:
-LMN injury involving CN XII-hypoglossal ipsilaterally.
-CST injury causing spastic paralysis contralaterally. |

|
Corticobulbar Tract 1. arises from ¨head¨portion of primary motor cortex
2. axons coarse through genu of the internal capsule
3. axons terminate (synapse) on the LMNs (cranial nerves) in the brain stem
4. Injury to this system superior to the Facial Nucleus (which is located in the pons) results in what neuro deficit? Contralateral Spastic Paralysis on the Lower muscles of facial expression.
|

|
contralat spastic paralysis for the lower muscles of facial expression.
From the interenet: LMN of brainstem receive bilat corticobulbar input. Unilat lesions have no effect on head/neck muscles clinically except those muscles which are bilat: 1) contralat lower facial paralysis, and 2) contral genioglossus tongue muscle (tongue deviates to affected side). Summary: a lesion involving all of the corticospinal and corticobulbar fibers from the left cerebral cortex produces
|
|
cerebellum
1.function - coordination of voluntary movement; monitors and compares intention and actual movement and sends out corrective feedback. 2.influences ipsilateral musculature
3. direct injury results in what deficits? ipsilateral ATAXIA
4. 3 segments of cerebellum & disorders. a) Flocculonodular lobe (vestibulocerebellum) - truncal ataxia. b) Anterior Lobe (spinocerebellum) - gait ataxia. c) Posterior Lobe (cerebrocerebellum) - -hypertonicity -intention tremor -dysmetria (past pointing) -dysdiodochokinesia (difficulty with RRAMs) -asynergia/dyssynergia (lack of smoothness) -dysarthria (difficulty with speech)
|


|
Posterior Lobe (cerebrocerebellum) of Cerebellum
|
|
1. Truncal ataxia - where is the disorder? Flocculonodulae Lobe of Cerebellum (Vestibulocerebellum)
2. Gait ataxia - -where is the disorder? Anterior Lobe of Cerebellum (Spinocerebellum) -involves input from what type of receptors? proprioceptors -in what population is this degeneration seen? alcoholics |
|
•Caudate Nucleus
•Putamen
•Globus Pallidus
•Subthalamic Nucleus
•Substantia Nigra

|
|
Basal Ganglia 1. Functions - muscle tone, posture, gross movement, programmed movement, cognitive aspect of movement and sequencing, suppress unwanted movement
2. Influence contralateral musculature.
3. Injury/Disease characterized by contralateral dyskinesias
4. Name 4 disorders of basal ganglia -Huntington's Chorea - abnormal involuntary writhing -Athetosis - continuous stream of slow, sinuous, writhing movements, typically of the hands and feet. -Ballismus/Hemiballismus -violent flinging motions of a limb or body part that tend to be more proximal than distal. -Parkinson's Disease - decreased stimulation of the motor cortex by the basal ganglia, normally caused by the insufficient formation and action of dopamine |
|
Parkinson's Disease 1. Disorder of what region - basal ganglia (decr stimulation from decr dopamine) 2. 5 clinical signs -lead pipe rigidity -akinesia (hesitancy initiating movement) -bradykinesia -rest tremors -masked expression
|

|
Pain Categories
1. Nocioceptive pain - tranduced from perepheral receptors that are being destroyed
2. Neuropathic Pain - damage to peripheral or central nerves (eg. Carpal Tunnel Syndrome, MS)
3. Acute - sharp & abrupt. Lasts minutes to weeks. Eventually dissapates if we can alleviate the cause.
4. Chronic - unresolved acute pain.
5. Learned - chronic pain that creates a circuitry of pain without external stimuli. |
|
Learned Pain 1. strong affective component (pt's mood) 2. generated by supraspinal centers 3. involves plastic changes within the CNS (responding to stimulation) |
|
Anterolateral System (ALS)
1. Transmits which modalities Protopathic (pain and temp) 2. Pain projector neurons (nociceptors) in dorsal horn of spinal grey can project to what 3 areas via what tracts to cause what response?
a) reticular formation via spinoreticular tract - in brainstem, consists of cells that modulate pain.
a) periaqueductal gray (PAG) via spinomesencephalic tract - in mesencephalon, gives us endogenous endorphines to shut off pain projection neurons at reticular formation; also, in situations of chronic stimulation can turn on pain progression centers in reticular formation to increase amount of pain.
c) Spinothalamic tract - thalamus projects to cortex, resulting in conscious perception of pain.
|
|
1) prior experience 2) context 3) emotion 4) frequency of stimulation = plasticity |
|
1) peripheral hypersensitivity - lower sensitivity of dorsal root primary afferent neurons
2) central hypersensitivity - pain projection neurons - reticular formation - periaquaductal grey - thalamus/hypothalamus - cerebral hemispheres (sensory cortex and frontal lobe to create personality changes) |
|
describe peripheral hypersensitivity causes of the ¨wind up¨of the CNS to transmit pain
Peristant stimulation of primary nociceptors causes... 1. activitation of dormant nociceptors in skin
2. threshold lowering of projection neurons, causing them to fire with less stimuli
3. conversion of multimodal dorsal horn neurons to pain projection neurons
4. degeneration of inhibitory interneurons that are normally stimulated by rubbing a painful area. |
|
2 results of peripheral hypersensitivity/plastic changes:
1. Allodynia - painful response to normally painless stimulation. 2. Spontaneous Pain/Spinal Memory |
|
Learned pain
General Anesthesia + Supplemental Spinal Block (to shut down spinal transmission for prevention of plastic changes).
|
|
1. Increased dendritic arborization 2. Increased sprouting of dendritic spines 3. Increased numbers of synapses |
|
1. Rostral Ventral Medulla (RVM) - pain modulation centers that have the ability to inhibit or excite dorsal horn pain projection neurons.
2. Periaqueductal Grey (PAG) - receives descending info from hypothal and cerebral cortices and sends excitatory input to RVM.
3. Thalamus - processes all sensory input (except olfaction) and relays to conscious level. |
|
Hypothalamus Frontal and Prefrontal cortices Insular cortex Limbic lobe Amygdala
.....are all structures sensitized by increased nocioceptive input & all project to the periaqueductial grey (PAG), which sends excitatory input to the Rostral ventral medulla (RVM), which can either inhibit or excite the dorsal horn pain projection neurons. |
|
Limbic Lobe - This structure is sensitized by increased nociceptive input and involves emotion.
Amygdala - This lays within the above structure and is involved in extreme/emphatic emotion.
(These two structures influence why people with pain are in severe emotional distress.) |

| There is no need for an external nociceptive stimulus b/c the pain pain pathway is so strong it functions on its own. |
|
Prevention Stop the source of the pain, which prevents plastic changes.
Treatment NSAIDS Dorsal Column stimulation (dorsal horn multimodal neurons can transmit pain or proprioception - treadmill training swtiches them back to proprioception) |
|
Pain transmission is decreased with increased propriospinal input.
Why? Dorsal horn multimodal neurons can transmit pain or proprioception. Chronic pain results in plastic changes of the conversion of the multimodal neurons to pain receptors. Treadmill training swtiches them back to proprioception. |
| 50% |
|
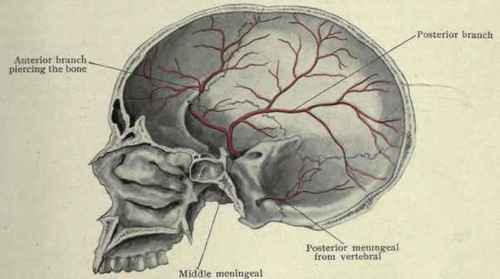
Middle Meningeal Artery - major arterial supply to the dura matter
Pathology: Epidural Hematoma has classic bulging inward shape.
|

|
Cerebral Bridging Veins - large veins that drain into the venous sinuses
|

 Pathology: Subdural Hematoma
Pathology: Subdural Hematoma 
|
A rupture of superficial branches of the anterior, middle, and posterior cerebral arteries causes a subarachnoid hematoma.
|

|
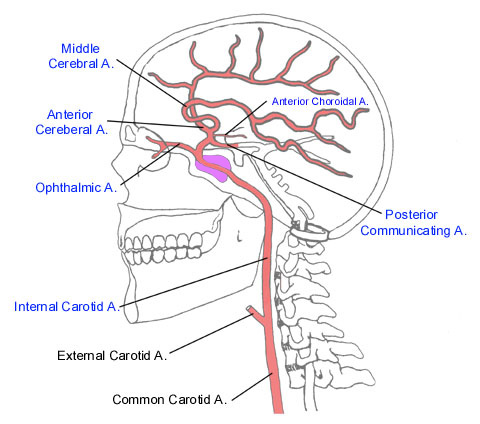
Internal Carotid System

|
 Vertebrobasilar System
Vertebrobasilar System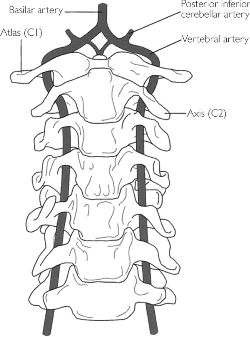

|
Internal carotid artery branches:
Note: Anterior and Middle Cerebral Arteries Supply the sensory and motor cortex!!!
|



|
Anterior Cerebral Artery Syndrome
REMEMBER: Anterior cerebral artery supplies the medial surface of the cerebral cortex as shown below:
|
 1. Contralateral hemiplegia or hemiparesis of the lower extremity
1. Contralateral hemiplegia or hemiparesis of the lower extremity
|
Middle Cerebral Artery Branches 1. Lenticulostriate Arteries: basal ganglia (bradykinesia, chorea), internal capsule, optic radiations
2. Cortical Branches to frontal, parietal, temporal lobes.
|



|
Middle Cerebral Artery Syndrome
3. Homonymous hemianopsia(L or R) (lenticulostriate a. branch supplies optic radiations) This is an example of L. Homonymous Hemianopsia 4. Aphasia: Left cerebral hemisphere
Supply of the Middle Cerebral Artery is lateral cerebral cortex. |


|
Vertibrobasilar System 1. vertebral artery system branches: -Anterior spinal artery
2. basilar artery branches: -Anterior inferior cerebellar artery
|


|
1. Bilateral sensory and motor signs
2. Inferior alternating hemiplegia (medulla) --contralateral hemiplegia of arm & leg (pyramid—corticospinal fibers) --contralateral loss position sense, vibration, discrim. touch (medial lemniscus) --deviation of tongue to ipsilateral side when protruded; muscle atrophy (CN XII hypoglossal nerve in medulla or CN XII nucleus)
3. Posterior inferior cerebellar artery (PICA) syndrome --contralateral body pain & temp loss (anterolateral system/spinothalamic tract) --ipsilateral face pain & temp loss (spinal trigeminal tract & nucleus)
4. Middle alternating hemiplegia (Pons)
--contralateral hemiplegia of arm & leg (corticospinal fibers in basilar pons) --contralateral loss/decrease of proprioception, vibration, discriminative touch (medial lemniscus) --ipsilateral lateral rectus muscle paralysis (abducens nerve fibers or nucleus—CN 6) 5. Posterior cerebral artery syndrome I looked this up, not it lecture, 99% sure its not on test b/c lecturer said nothing about it. This syndrome results from bilateral medial thalamic infarction. Patients vary from lethargic to obtunded to comatose, but in some cases may be agitated and may have associated hemiplegia or hemisensory loss. Occasionally, the cranial nerve III nucleus is involved, with resultant ophthalmoplegia. -Unilateral infarction produces homonymous hemianopia. -Bilateral infarctions of the occipital lobes produce varying degrees of cortical blindness depending upon the extent of the lesion. -Occlusion of the posterior choroidal artery may produce a distinct syndrome of hemianopia, hemidysesthesia, and memory disturbance due to infarction of the lateral geniculate, fornix, dorsomedial thalamic nucleus, and posterior pulvinar. |
|
1. Anterior Cerebral Arteries (2), anterior communicating artery, internal carotid arteries (2), posterior communicating arteries (2), posterior cerebral arteries (2)
2. Completely formed in 20% of population
|
