1. Bilateral sensory and motor signs
2. Inferior alternating hemiplegia (medulla)
--contralateral hemiplegia of arm & leg
(pyramid—corticospinal fibers)
--contralateral loss position sense, vibration, discrim. touch
(medial lemniscus)
--deviation of tongue to ipsilateral side when protruded; muscle atrophy
(CN XII hypoglossal nerve in medulla or CN XII nucleus)
3. Posterior inferior cerebellar artery (PICA) syndrome
--contralateral body pain & temp loss
(anterolateral system/spinothalamic tract)
--ipsilateral face pain & temp loss
(spinal trigeminal tract & nucleus)
4. Middle alternating hemiplegia (Pons)
--contralateral hemiplegia of arm & leg
(corticospinal fibers in basilar pons)
--contralateral loss/decrease of proprioception, vibration, discriminative touch
(medial lemniscus)
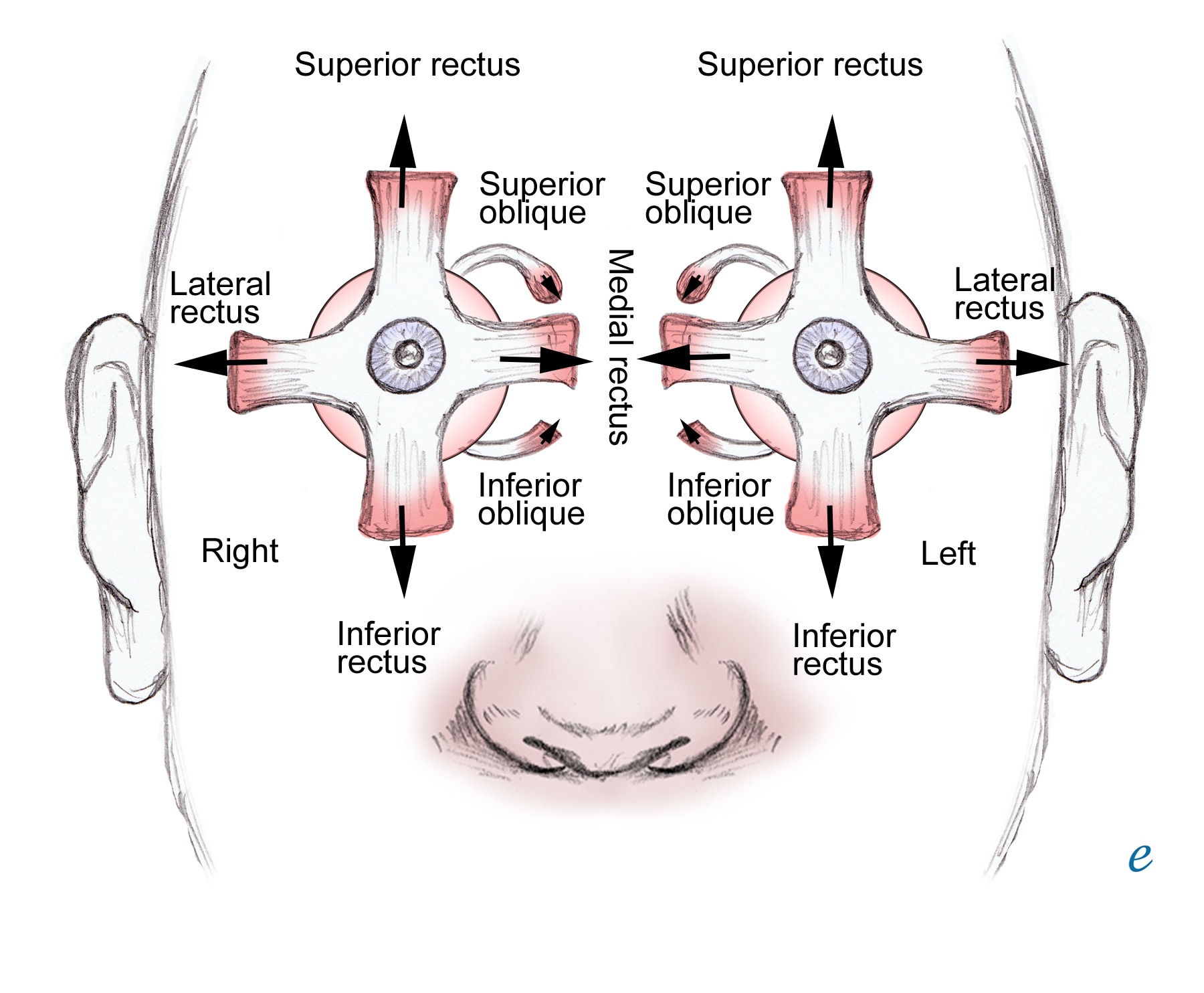
--ipsilateral lateral rectus muscle paralysis
(abducens nerve fibers or nucleus—CN 6)
5. Posterior cerebral artery syndrome
I looked this up, not it lecture, 99% sure its not on test b/c lecturer said nothing about it. This syndrome results from bilateral medial thalamic infarction. Patients vary from lethargic to obtunded to comatose, but in some cases may be agitated and may have associated hemiplegia or hemisensory loss. Occasionally, the cranial nerve III nucleus is involved, with resultant ophthalmoplegia.
-Unilateral infarction produces homonymous hemianopia.
-Bilateral infarctions of the occipital lobes produce varying degrees of cortical blindness depending upon the extent of the lesion.
-Occlusion of the posterior choroidal artery may produce a distinct syndrome of hemianopia, hemidysesthesia, and memory disturbance due to infarction of the lateral geniculate, fornix, dorsomedial thalamic nucleus, and posterior pulvinar.



























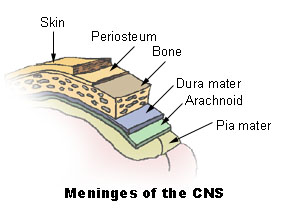
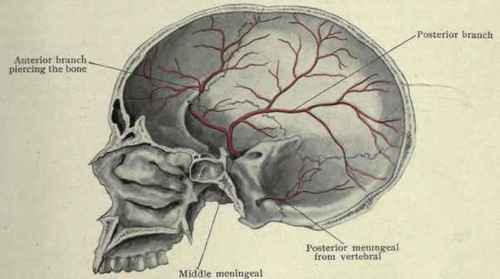


 Pathology: Subdural Hematoma
Pathology: Subdural Hematoma 

 Vertebrobasilar System
Vertebrobasilar System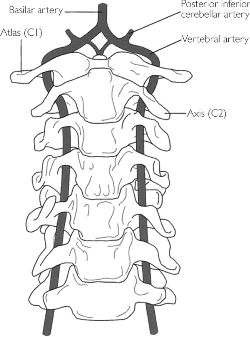





 1. Contralateral hemiplegia or hemiparesis of the lower extremity
1. Contralateral hemiplegia or hemiparesis of the lower extremity







